As mentioned in the last blog post, the impacts of alcohol on the growing fetus can be controlled by the genes. It is widely known that the symptoms of all the disorders that fall under the title Fetal Alcohol Spectrum Disorder fall on a gradient. However, there is not a lot of grey area in regards to prenatal alcohol exposure; the mother either drinks or she doesn’t. A child can’t be sort of exposed to alcohol in utero, the same way a woman can’t be sort of pregnant. The question then is, why is there a gradient when of symptoms when the actual exposure is so definitive? A study done by Hemingway et al. looks at the effects of fetal genetics in cases of FASD in an attempt to answer this question. If two fetuses were exposed to the same level of alcohol at the same time during pregnancy, but showed vastly different symptoms, it would have important implications for public health and education surrounding maternal drinking. The purpose of this study was to compare ranges of FASD symptoms among four groups; identical twins, fraternal twins, full siblings and half siblings sharing the same birth mother. The study was attempting to do the following four things;
- Determine if the prevalence of FASD was higher among fraternal twins compared to identical.
- To determine if the prevalence of FASD increases with the decrease in shared genetic material between sibling pairs.
- Document the greatest difference between twin pairs with identical Prenatal Alcohol Exposure (PAE). Can twins with identical PAE be at the opposite ends of the FASD spectrum?
- Estimate the heritability of the FASD phenotypes (the physical presentation of the symptoms)
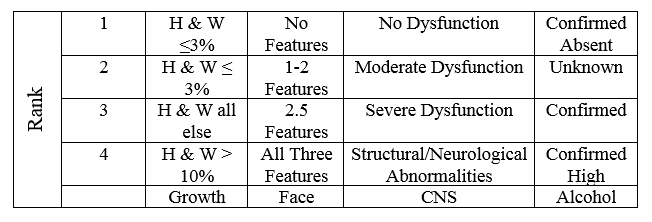
The presence of FASD among the sibling pairs was evaluated based on the following criteria (in the presented order);
- Growth deficiency
- FAS facial phenotype (thin upper lip, wide set eyes, etc)
- CNS structural or functional abnormalities (behavioural disorders, misculoskeletal issues, etc)
- PAE
The degree of each feature was ranked on a four-point scale. 1 is the absence of the criteria, and 4 is a strong, “classic” presentation of the FAS phenotype.
The siblings were placed into four groups;
- Monozygotic twins (identical twins, share 100% of their genome)
- Dizygotic twins (fraternal twins, share ~50% of their genome)
- Full- siblings (share ~50% of their genome)
- Half-siblings sharing a common mother (share ~25% of their genome)
The results showed the proportion of sibling pairs with FAS was very similar to the proportion of their genome they shared; all the monozygotic twin pairs shared FASD, 56.4% of the dizygotic twin pairs shared FASD, 40.7% of full siblings and 22.2% among half siblings. This represents a linear decrease with the proportion of genome shared. There was no information that suggested gender impacted the diagnosis of FASD.
Although the diagnosis of FASD was present in the approximate proportion as the shared genome, it did not always present itself to the same degree. The concordance (similarity) between the dizygotic twins was extremely varied. One twin could experience low to moderate symptoms of FASD, while the other could experience severe symptoms as reported by the four-point scale. The full-siblings pairs and half-sibling pairs also experienced large ranges of the FASD phenotypes.
Despite the difference in the FASD presentation, both monozygotic and dizygotic twin pairs had a 100% heritability rate. This means that the presence of FASD was entirely due to their genome (despite the differences in phenotype) and not due to environmental risk factors.
The results of this study support the idea that fetal genetics can impact the impacts of prenatal alcohol exposure. The prevalence of FASD among the sibling pairs was directly correlated with how much of their genome was shared between them. Similar studies done over the years, both on twins and on model animals, with FASD has also presented with similar results. This suggests that there is a genetic component to FASD. Although the genes may influence the presentation of the symptoms, they can not cause them.
It gives further support to the fact that FASD in all its forms is 100% preventable. The answer to the question; What is a safe amount of alcohol to drink while pregnant? Has a very simple answer: nothing at all.
Article Reference
Hemingway, S.J.A., J.M. Bledsoe, J.K. Davies, A. Brooks, T. Jirikowic, E.M. Olson & J.C. Thorne (2019). Twin study confirms virtually identical prenatal alcohol exposures can lead to markedly different fetal alcohol spectrum disorder outcomes- fetal genetics influences fetal vulnerability. Advances in Pediatric Research. 5(23).